
Inpatient vs Outpatient Medical Coding: Key Differences Explained
Introduction: Two Worlds of Medical Coding
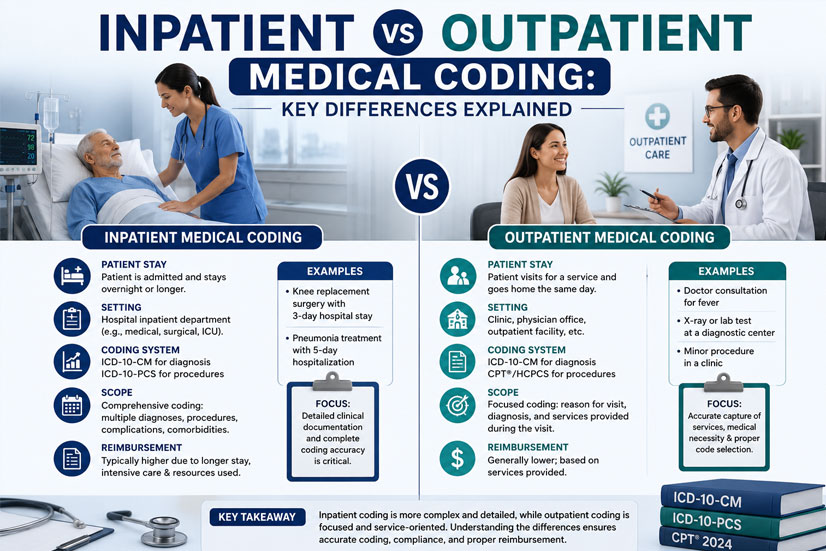
Medical coding is not a one-size-fits-all profession. One of the most fundamental distinctions you'll encounter is between inpatient and outpatient coding. Whether you're preparing for an interview, CPC exam, or your first job, understanding these differences is critical. Inpatient coding refers to patients who are formally admitted to a hospital, typically staying overnight or longer. Outpatient coding covers patients who receive care without being admitted — think clinic visits, emergency department stays, outpatient surgeries, and observation services.
Why does the distinction matter? Because coding guidelines, code sets, payment methodologies, and the level of detail required differ dramatically between these two settings. Choosing the wrong code set or applying inpatient rules to an outpatient record (or vice versa) leads to claim denials, compliance risks, and revenue loss. Let's break down the key differences every coder must know.
1. Code Sets Used: ICD-10-CM/PCS vs CPT/HCPCS
Inpatient coding (hospital inpatient, long-term acute care) primarily uses ICD-10-CM for diagnoses and ICD-10-PCS (Procedure Coding System) for inpatient procedures. ICD-10-PCS is a highly specific, 7-character alphanumeric code set used exclusively for hospital inpatient procedures. It captures details like approach, device, and body part with incredible precision.
Outpatient coding (physician offices, hospital outpatient departments, ambulatory surgical centers) uses ICD-10-CM for diagnoses (same as inpatient) but uses CPT (Current Procedural Terminology) and HCPCS Level II for procedures and services. CPT codes describe medical, surgical, and diagnostic services and are used by both hospitals (for outpatient billing) and physicians. This is a major difference: inpatient procedures = ICD-10-PCS; outpatient procedures = CPT/HCPCS.
2. Payment Systems: MS-DRG vs APC
The financial side of coding varies completely. Inpatient hospital stays under Medicare (and many commercial payers) are paid under the Inpatient Prospective Payment System (IPPS) using MS-DRGs (Medicare Severity Diagnosis Related Groups). Each MS-DRG has a fixed payment amount based on the principal diagnosis, complications, and procedures. Coders directly impact DRG assignment.
Outpatient hospital services are paid under the Outpatient Prospective Payment System (OPPS) using APCs (Ambulatory Payment Classifications). Each service (CPT/HCPCS code) is assigned to an APC, which determines reimbursement. Physician office coding uses the Physician Fee Schedule (PFS) based on RVUs (Relative Value Units). Understanding these payment models is key for interview questions.
3. Documentation and Coding Guidelines
Inpatient coding follows the Uniform Hospital Discharge Data Set (UHDDS) definitions. Principal diagnosis is defined as "the condition established after study to be chiefly responsible for the admission." Secondary diagnoses require specific criteria (e.g., clinical evaluation, therapeutic treatment, increased length of stay). Present on Admission (POA) indicators are required for all diagnoses.
Outpatient coding follows different rules. For example, the Outpatient Prospective Payment System (OPPS) has guidelines for "significant procedure" reporting. Outpatient coders use different definitions for "primary diagnosis" versus "principal diagnosis." Also, POA reporting is not required in outpatient settings except for certain quality measures. Coders must know which rules apply to their setting.
4. Coding Depth and Complexity
Inpatient coding generally requires deeper clinical knowledge. Coders must be able to interpret entire medical records (history & physical, progress notes, operative reports, discharge summaries). They identify all documented conditions that meet UHDDS definition of "other diagnoses." Inpatient coders often specialize in high-acuity areas like ICU, NICU, or transplant.
Outpatient coding is often more focused on the reason for the specific encounter. An office visit for knee pain would focus on that problem. However, outpatient coding has its own complexities: correct Evaluation & Management (E/M) leveling, modifier usage (-25, -59, -XU), and bundling rules (NCCI edits). Outpatient coders must master CPT procedure coding, which differs from ICD-10-PCS.
5. Common Documentation Sources
Inpatient coders primarily work with the Discharge Summary, full Operative Report (if surgery occurred), daily Progress Notes, Consultation reports, and lab/radiology results. The entire hospitalization is considered as a single "episode of care." Outpatient coders work with Clinic Notes, Emergency Department Records, Ambulatory Surgery Reports, and Procedure Notes. Each outpatient encounter is a separate, distinct episode.
This difference affects coding workflow. An inpatient coder might code a 20-day stay with multiple procedures and complications. An outpatient coder might code 30 different patient visits in the same day. Time management and focus areas differ significantly.
6. Certification and Career Paths
Certifications matter. For inpatient hospital coding, the AHIMA credentials are often preferred: CCS (Certified Coding Specialist) or RHIT/RHIA. For outpatient and physician coding, the AAPC credentials like CPC (Certified Professional Coder) are widely recognized. Many coders eventually earn both. Some hospitals require inpatient coders to pass an ICD-10-PCS proficiency exam.
Your career direction depends on which setting you prefer. Inpatient coders often work for hospitals, health systems, or inpatient coding vendors. Outpatient coders work in physician practices, hospital outpatient departments, ambulatory surgery centers, or remote coding roles. Some coders specialize further (e.g., emergency department coding, same-day surgery coding).
Quick Comparison Table
Common Interview Questions on This Topic
Expect questions like: "What code set would you use to code an inpatient colonoscopy? An outpatient colonoscopy?" (Inpatient: ICD-10-PCS; Outpatient: CPT). "Explain the difference between MS-DRG and APC." Or "A patient is in observation status for 24 hours — inpatient or outpatient?" (Observation is generally outpatient, even if it spans midnight, unless formal inpatient admission order is written).
Another classic: "If a hospital inpatient has a procedure done, which code set captures that procedure?" (ICD-10-PCS, not CPT). Knowing these distinctions shows employers you understand real-world coding workflows.
Conclusion: Choose Your Path or Master Both
Inpatient and outpatient coding are distinct specialties within medical coding. Inpatient coding demands deep knowledge of ICD-10-PCS, MS-DRGs, and complex clinical scenarios. Outpatient coding focuses on CPT/HCPCS, E/M coding, modifiers, and payer-specific rules. Many coders start in outpatient roles (e.g., physician office) and transition to inpatient after gaining experience and additional credentials.
Whichever path you choose, understanding both sides makes you a versatile, valuable coder. For interviews and exams, memorize the core differences: code sets (ICD-10-PCS vs CPT), payment systems (MS-DRG vs APC), and documentation rules (POA vs no POA). With this knowledge, you'll confidently answer questions and excel in your medical coding career.
Ready to test your knowledge? Take a sample operative report for a total knee replacement. Code it as inpatient (using ICD-10-PCS) and then as outpatient (using CPT). Compare the code structures — that's the difference in action!